Agencies, contracts, and clinic logistics had been unfamiliar at first - but they were still written in a language we could learn. When our first PGT-A reports arrived, we felt something different. This was biology at a level we had never needed before, attached to decisions about future children.
The pages were full of terms we had to look up: euploid, aneuploid, mosaic, monosomy, trisomy, and embryo grades like 4BA and 5AB. Some of those words eventually became part of our own surrogacy vocabulary; others were the kind of terms we wished had been gathered in one simple glossary from the beginning.
There were also sex results - XX and XY - which felt strangely concrete in a document that was otherwise abstract.
We are not scientists. We are intended parents trying to understand enough to ask sensible questions, follow our clinic’s guidance, and not panic at words we had never seen on a spreadsheet before.
This is not an article about becoming geneticists. It is about what we learned when we had to read our PGT-A results for the first time - what the test is, what the grades mean, what euploid and mosaic actually imply, and where the limits of the report are.
We are intended parents sharing our experience, not medical or legal advisors. This is not medical advice, not a guide to every lab’s reporting format, and not a recommendation that everyone should choose genetic testing. It is simply how we learned to read our PGT-A results, and what we wish someone had explained in plain language before the first report landed in our inbox.
The first stage where we felt completely outside our comfort zone
Surrogacy had already asked us to learn new vocabulary: gestational carrier, intended parent, blastocyst, transfer window, and dozens of administrative terms tied to contracts and travel.
Genetics felt like a different category. It was not only unfamiliar. It carried weight. Each line on the report seemed to point toward a possible future child - or toward an embryo our clinic might advise us not to transfer.
This was the first stage where surrogacy stopped being logistics and became biology in a way we did not feel prepared for. We had chosen an egg donor, created embryos, and entered the waiting period after biopsy. When results returned, we opened PDFs that looked clinical and precise, while we still needed a glossary beside us.
Understanding the report was not optional curiosity. It was part of participating responsibly in our own process.
What is PGT?
PGT stands for Preimplantation Genetic Testing. It is testing performed on embryos before transfer into a uterus - whether that uterus belongs to an intended parent or a gestational carrier.
In our route, testing happened at the blastocyst stage: roughly five to seven days after fertilization, when the embryo has developed into a hollow ball of cells with two distinct parts. A small sample of cells is taken, usually from the outer layer called the trophectoderm (the part that will eventually help form the placenta). Those cells are sent to a genetics laboratory for analysis.
The purpose, at a high level, is to learn something about the embryo’s chromosomal status before anyone commits to a transfer. Clinics may use this information to help prioritize embryos, discuss risks, and plan next steps. Different types of PGT look for different kinds of problems - which is why the letters after “PGT” matter.
Our reports used PGT-A with next-generation sequencing (NGS). At a high level, that means the lab analyzes DNA from the trophectoderm sample to screen for detectable chromosomal imbalance - aneuploidy - not for every genetic disease or condition. The biopsy captures a small sample of cells, not the entire embryo. Some changes may not be detected, depending on the technology and what is being tested. No test can guarantee chromosomally normal offspring, and PGT-A does not replace prenatal screening or medical follow-up during pregnancy where that applies.
We are not describing laboratory procedures in detail here. Biopsy technique, freezing protocols, and turnaround times vary by clinic. What mattered to us as intended parents was simpler: a sample was taken, a report came back, and we needed to know what the words on that report meant - and what they could not tell us. Final interpretation belongs to physicians and, where appropriate, genetic counselors.
PGT-A, PGT-M, PGT-SR, and bundled panels
Not all preimplantation genetic testing is the same. The suffix tells you what kind of question the lab is trying to answer.
Our clinic offered PGT-A as an optional add-on for our situation. Other families need different tests because of known genetic conditions or structural chromosome issues. The table below is a simplified comparison - routes and clinic menus differ, and qualified professionals should explain what applies to you.
| Test | What it looks for | Who often uses it |
|---|---|---|
| PGT-A | Whether the embryo has the expected number of chromosomes (aneuploidy screening) | Common optional add-on in IVF and surrogacy; often discussed with advanced maternal age, repeated loss, or multiple embryos to compare |
| PGT-M | A specific known monogenic disorder (single-gene condition) in the family | Intended parents who are carriers of or affected by a defined inherited condition and need to test for that gene |
| PGT-SR | Structural rearrangements of chromosomes (for example translocations) | People with a known chromosomal rearrangement who need embryos screened for balanced vs unbalanced outcomes |
| Bundled / expanded panels | Varies by lab - may combine aneuploidy screening with additional analysis under names such as PGT-Complete or similar | Clinics that offer expanded packages; scope is not standardized across labs, so ask what is actually included |
For us, PGT-A was the relevant category. We did not have a single known gene mutation to target (PGT-M) or a structural rearrangement to screen for (PGT-SR). We wanted a chromosomal overview of each embryo before transfer planning moved forward.
Some clinics offer bundled or expanded panels under names such as PGT-Complete. The exact scope depends on the lab, so the important question is what is actually included - not the marketing label alone.
The existence of several PGT types is a reminder that “genetic testing” is not one universal product. Ask your clinic which test is actually being ordered and what it can and cannot detect.
Why we chose PGT-A
We chose PGT-A for a few practical reasons - none of which should be read as a universal recommendation.
First, we wanted to know each embryo’s chromosomal status before transfer decisions. Surrogacy already involved many moving parts; we preferred not to transfer without that information when our clinic offered it.
Second, our reports included sex information - XX or XY - which mattered for our personal planning across two gestational-carrier paths. We are planning for two children with two carriers, and knowing sex helped us think about balance and timing. That was a personal planning preference for our situation, not a recommendation, and not something every clinic or country handles the same way.
Third, we understood that PGT-A may help a clinic prioritize embryos and may reduce the likelihood of transferring embryos with detectable chromosomal abnormalities. It could not, by itself, guarantee implantation, pregnancy, birth, or a chromosomally normal child. No report replaces the steps that still lie ahead after a transfer.
Some intended parents decline PGT-A for cost, timing, philosophical reasons, or clinic advice. That is a valid path. We are describing our choice, not advocating for one approach over another.
PGT-A also introduced a budget uncertainty we had not fully anticipated. Many surrogacy costs feel fixed, or at least predictable once quoted. PGT-A is often priced per embryo tested - and we did not know in advance how many embryos we would end up with. We could budget the approximate price per embryo (around $500 in our case), but not the final number of embryos. Because we were planning two pregnancies across two gestational-carrier paths, the total could move noticeably depending on how many blastocysts survived to biopsy. That was not a complaint. It was a planning lesson: costs vary by clinic, country, lab, and package, and per-embryo testing makes the total harder to pin down early.
We could budget the price per embryo, but not the final number of embryos.
That budget lesson sat beside the bigger medical lesson: even after paying for more information, the result was still information, not certainty.
PGT-A gave us selection information. It did not guarantee implantation, pregnancy, or a baby.
How embryo grading works
Before we even opened the genetics section, each embryo already had a morphology grade from the embryology lab. That grade describes how the embryo looked under the microscope. The PGT-A result describes chromosomal status detected in the trophectoderm biopsy. They are related in conversation, but they are not the same measurement.
A pretty-looking embryo can be aneuploid. A euploid embryo can have a less impressive morphology grade. Our clinic weighed both - along with factors we could not see on the report alone.
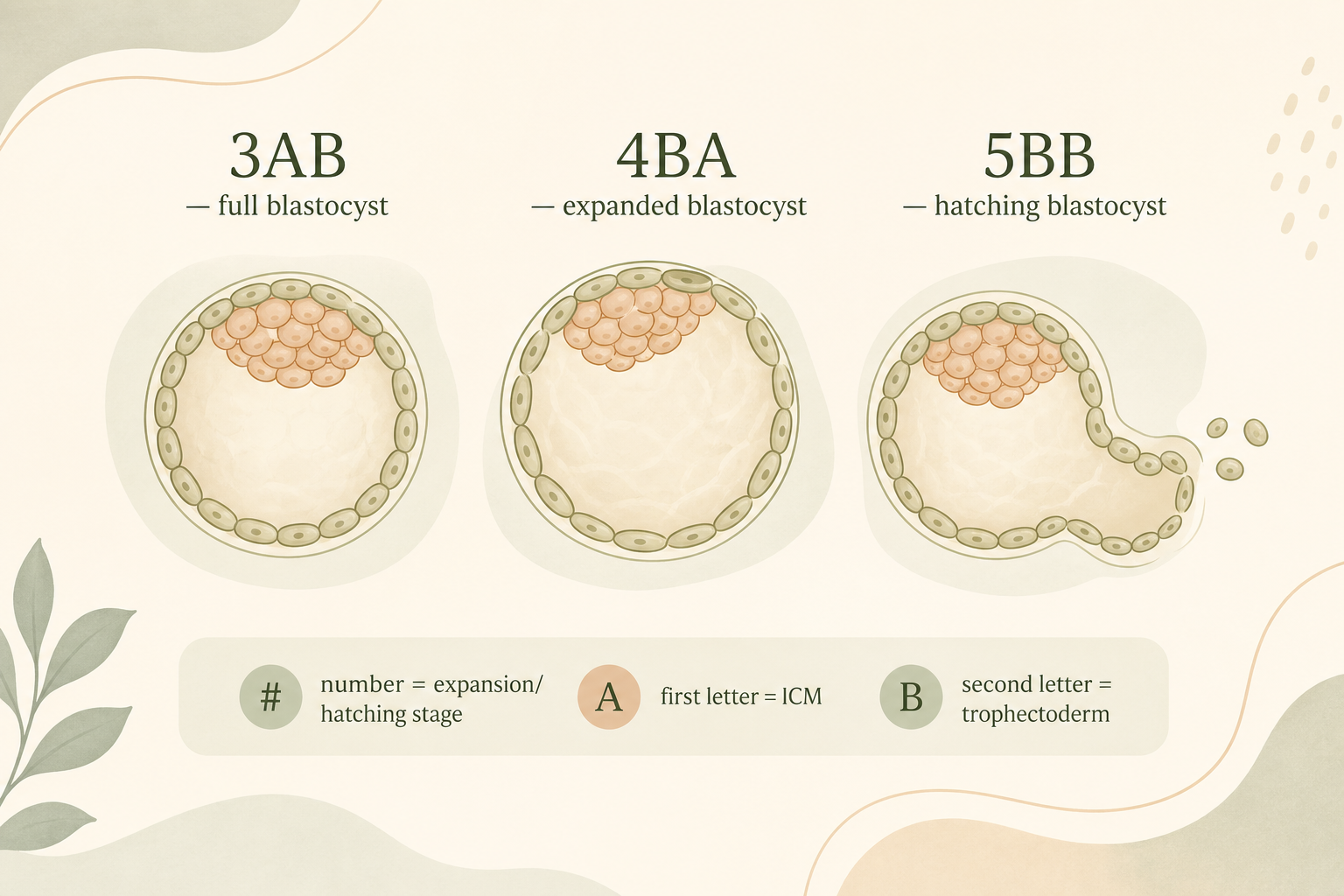
The format we saw most often was a number followed by two letters, such as 3AB, 4BA, 4BB, 5AB, or 5BB. This follows the common Gardner-style blastocyst grading system, though labs may vary slightly.
The number refers to expansion and hatching stage - how far the blastocyst has developed. In the scale we saw most often: 3 is a full blastocyst, 4 is expanded, 5 is hatching, and 6 is hatched. Stage 5 is not the same as fully hatched; that is closer to stage 6.
The first letter grades the inner cell mass (ICM) - the cluster of cells that will eventually form the fetus. An A typically means high quality, B good, and C lower quality by visual assessment.
The second letter grades the trophectoderm - the outer cell layer (the same region often sampled for PGT-A). Again, A is generally strongest and C weakest on the lab’s visual scale.
So 3AB might describe a full blastocyst with strong ICM and trophectoderm grades. 4BA might describe an expanded blastocyst with a very good trophectoderm grade and a good-but-not-top ICM. 5BB might describe a hatching blastocyst with solid but not top morphology in both categories.
Embryo grade is how the embryo looks. PGT-A result is what the genetics lab detected in the biopsy. We learned to read both without assuming one would always match the other.
How to read a typical report
Lab layouts differ, but most PGT-A reports we saw were organized like a table - one row per embryo. We are not reproducing our private results here. The table below is a fictional educational example only. Your clinic’s layout, column names, and wording may differ.
Fictional example - not our real report
| Embryo ID | Embryo grade | PGT result | Sex | Interpretation |
|---|---|---|---|---|
| Example A | 5AB | Euploid | XX | Normal chromosome number detected |
| Example B | 4BA | Low-level mosaic | XY | Mixture of normal and abnormal cells; requires clinic interpretation |
| Example C | 4BB | Aneuploid | - | Chromosome imbalance detected; clinic to advise on next steps |
Embryo ID is the lab’s identifier - often matching the label your clinic uses internally. Embryo grade is the morphology score from embryology. PGT result is the genetic classification. Sex is determined from the chromosomes (XX for female, XY for male) when the result is clear enough to report. Interpretation is the plain-language summary, though the technical result line is the one physicians usually discuss in detail.
When we first opened a real report, we read the interpretation column first because it felt approachable. Then we learned to read the PGT result line itself and bring questions back to our clinic rather than treating the summary as the final word.
Real reports may include chromosome details such as +21, -X, dup, del, or [mos]. Those shorthand codes need clinic interpretation. At a simple level: + often indicates an extra chromosome (trisomy), - a missing chromosome (monosomy), dup a duplication, del a deletion, and [mos] mosaicism. We learned not to decode those strings alone.
Some summary reports also combine embryo quality, PGT result, sex, interpretation, and embryo development counts in one view - similar columns to the fictional table above, but with lab-specific formatting.
A report is a map, not a destination. Our clinic still had to help us decide what to do with it.
When the report became a conversation
Reading the PDF alone only got us so far. After our PGT-A results arrived, we joined a call with the clinic’s genetics specialist. The purpose was straightforward: explain the reports in plain language, answer our questions, and discuss what the results might mean for transfer planning.
Our agency was on the call as well - partly to help translate if needed, and partly to add practical context from journeys they had seen before. That combination mattered. The geneticist could explain what euploid and mosaic meant in our specific reports. The agency could help us understand how those results might fit into the wider surrogacy timeline we were already managing.
That call was where the report stopped being a PDF on a screen and became a decision conversation. We still did not make transfer choices alone afterward, but we arrived at those discussions with better questions and less guesswork.
The report gave us vocabulary. The genetics call helped us use it.
Euploid, aneuploid, and mosaic
This was the heart of the learning curve for us. Once we understood these terms, the rest of the report felt less like a foreign language.
Euploid means the embryo appears to have the normal number of chromosomes for a human embryo tested this way - typically 46 chromosomes in the analyzed sample. In plain terms: the chromosome count looks correct. Clinics may prioritize euploid embryos for transfer, but that is a medical judgment - and “euploid” still does not mean guaranteed pregnancy (more on that below).
Aneuploid means an abnormal number of chromosomes. You may also see specific terms like monosomy (one chromosome missing from a pair) or trisomy (an extra chromosome in a pair). Common examples appear in general education materials - for instance trisomy 21 is associated with Down syndrome. Transfer decisions for aneuploid embryos belong to your clinic; policies vary.
Mosaic sits between those clearer categories. A mosaic embryo has a mix of normal and abnormal cells in the sample tested. Labs often distinguish low-grade mosaic from high-grade mosaic, based on what proportion of cells appear abnormal. One lab we read defined low-grade mosaic as roughly 20–40% abnormal cells and high-grade mosaic as roughly above 40% up to 80% - but cutoff percentages depend on the laboratory, and mosaic transfer decisions are never simple.
Mosaic results can be the hardest to interpret without a physician. Some low-grade mosaic embryos may be discussed for transfer under specific guidance. High-grade mosaic or complex abnormal results - where multiple chromosome problems are involved - are generally reviewed more cautiously. There is no one-size-fits-all rule we could safely summarize here.
You may also see No result (sometimes Sin resultado in Spanish-language reports). That usually means the lab could not obtain a reliable result from the sample - reasons can include sample or DNA quality. Clinics may discuss re-biopsy, retesting, or treating the status as unknown rather than euploid or aneuploid.
We deliberately avoid alarmist language here. These labels describe chromosomal patterns in a small biopsy sample. They are not moral judgments about an embryo, and they are not predictions you should interpret alone at midnight with a search engine.
Our job as intended parents was to understand the vocabulary well enough to have a serious conversation with our clinic - not to become the final authority on our own report.

Why euploid does not mean guaranteed success
This mattered emotionally. It is easy to treat a euploid result like a green light that turns the rest of the journey into a formality. That is not how it works.
A euploid embryo can still fail to implant. A pregnancy can still miscarry. A transfer can still be cancelled or delayed for reasons unrelated to the PGT line - uterine lining, timing, medical hold, logistics between countries, or a gestational carrier’s cycle.
PGT-A also has technical limits. It tests the trophectoderm sample that was biopsied, not every cell in the embryo. It screens for detectable chromosomal imbalance in the way that specific NGS test is designed to do - not for every genetic condition, not for every structural problem, and not for everything that could affect a future child’s health. Some forms of polyploidy, uniparental disomy, balanced rearrangements, or very small changes may not be detected, depending on the technology used.
We found it helpful to reframe euploid as selection information, not as a promise. It gave our clinic one more data point. It did not remove grief, waiting, or the ordinary uncertainty of surrogacy. Embryo selection remains at physician discretion - and if pregnancy occurs, conventional prenatal testing and follow-up may still be recommended.
PGT-A gave us selection information. It did not guarantee implantation, pregnancy, or a baby.
How selection was discussed with the clinic
Intended parents do not truly choose embryos alone. The clinic has the final medical say - what is medically acceptable to transfer and what is not. We could express preferences, including sex preference where allowed and available in our route, but only when medically reasonable. Our preferences could shape the conversation; they did not replace the clinic’s responsibility.
For readers staring at a report for the first time, it may still help to know how we learned to read the page before those clinic discussions:
First, the PGT result - euploid, aneuploid, or mosaic - because that told us whether an embryo was even in the conversation for transfer.
Second, the embryo grade, as a tie-breaker among euploid options when several looked viable on paper.
Third, practical factors our clinic weighed with us: sex information for our two-carrier plan (where allowed), freezing dates, which gestational carrier was ready, and any mosaic case that needed deeper review.
In our situation, sex preference mattered because we were planning two children through two gestational carriers - not as a primary reason for choosing PGT-A, and not as something every clinic or country handles the same way. When two embryos were close enough in medical ranking, a preference could sometimes be considered. When the embryo matching our preference sat much lower in the clinic’s ranking, the clinic said no and prioritized the embryo with better expected success. We are not sharing real rankings or case details here; the pattern was simply that medical prioritization came first.
Finally, we waited for the clinic’s medical decision. The report gave us language. The clinic made the medical call, informed by experience, our history, and details we could not see on a PDF.
If you are looking at mosaic or complex results, that clinic conversation is not optional polish. It is the point where general education ends and personal medical guidance begins.
Read the report carefully. Share your preferences honestly. Let the clinic make the medical call.
What we carry forward
Reading PGT-A results was the first part of surrogacy that felt like stepping into a biology class we had never signed up for. It was also one of the most useful. Once we understood embryo grades, euploid and mosaic language, and the limits of the test, we could sit in physician meetings with better questions and less free-floating fear.
We still relied on our clinic for every transfer decision. We still treated euploid as hopeful information, not a guarantee. And we still remembered that genetics was only one chapter in a longer story that included donors, gestational carriers, contracts, travel, and waiting - lots of waiting. PGT-A gave us selection information; it did not replace the professionals who helped us use it.
If you are earlier in the journey, our article on how we chose an egg donor covers the profile stage that precedes embryo creation. Our piece on how we chose our two gestational carriers describes what came after we had embryos to think about transferring. And our first trip to Colombia is where the medical side of the process first became real on the ground.
Disclaimer
MySurrogacy does not provide medical, legal, tax, immigration, or financial advice. This article reflects intended-parent experience and is meant for general planning support only. Routes, clinics, and laboratory reporting formats vary; qualified professionals who know your situation should interpret your PGT results and advise on transfer decisions.